(Bogota, Montería, Colombia: June, 1997:) Our first stop was way out in the mountain jungles in a township called Guateque. From Guateque we traveled the muddy, washed-out roads to El Oscuro township. Because of the nearly daily downpours of rain, the roads were impassable except via donkeys, horses, and four-by-four rigs. The soil was a red clay that was very sticky and slick when mixed with water, and there was no gravel or decomposed granite base under any of the roadways. So where large amounts of water were running across the dirt roads, there was likely not to be any bottom to them.
In El Oscuro we assessed a very rural clinic. Across the roadway was the farm of one of the leading villagers. The dirt-floored, thatched-roofed house had no doors or windows but had plenty of chickens, ducks, turkeys, and pigs running through the house. The walls of the house were papered with pages out of old magazines in an apparent effort to keep the dust from blowing through them during the dry summer months. Large sheaves of rice hung from the rafters to dry. Before we left the primitive farmhouse we were served—and were expected to eat—some fresh coconut pudding and coffee, which I was dead certain were both made with bad water.
San Isidro was our next stop on our mountain tour. Rebecca Lupes is the township health-care provider and midwife. She is not a doctor or a nurse but does run the local clinic, except when the traveling government doctor comes around on Tuesdays and Thursdays. The clinic serves well over three thousand people and is very busy. Project C.U.R.E. can really help out just by sending a dental chair and a dental X‑ray machine. If those were in place, Rebecca felt she could get a dentist to periodically come to the township to help.
Other than the terribly obvious things needed in San Isidro, Rebecca requested first-aid kits for the other villages in the township, weight scales for children and adults, and a battery-operated megaphone of some sort to announce to the villages when the doctor was to arrive. There are no medical supplies, no oxygen facilities, no intravenous supplies or equipment, no medicine, and no sutures. They desperately need medicine to treat parasites, lice, ringworm, skin diseases, respiratory problems, and diarrhea. Other than having nothing, they are in great shape.
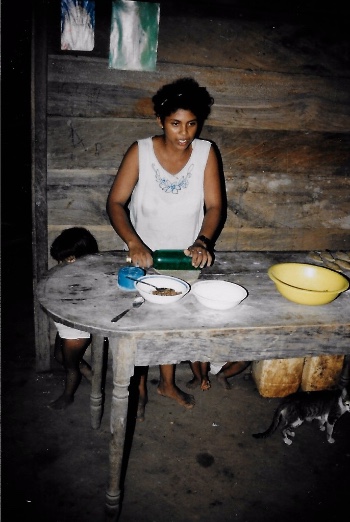
Our delegation stayed in San Isidro, and Father Bernie performed Mass for the township. The little chapel was packed out, and Justin and I had to sit right up front facing the congregation after being introduced as Project C.U.R.E. people. Rebecca, her mother, and her entire extended family prepared food for us to eat before we left to drive back to Montería. I took a picture of Rebecca in her kitchen preparing rice, yucca, soup, and a garden salad for us. Again, the homes had no doors, windows, or walls … mostly just thatched roofs and privacy walls around some of the bedrooms. The outside wall of Rebecca’s kitchen was a low fence. On the other side of the fence was a muddy pen where pigs, chickens, and goats were all sloshing around. The water used in the kitchen was caught from the roof in a moss covered concrete container. We all sat down and ate the food and drank the coffee. I prayed a lot!
On our way back to the city, we made one more rural stop. A young couple with a house full of kids was doing a grand job of running a farm of banana trees, passion-fruit trees, maize, guava, and other crops. We went into the kitchen, where the young mother was making cookies. I watched with amazement. She was rolling out the dough with an old, slender bottle.
There was a fire on the dirt floor right in the kitchen area. She had a big black kettle sitting on the floor, with three logs burning, one on each of three sides. On the floor next to the logs was a piece of sheet metal with another fire going on it. She would cut out the round cookies, place them side by side inside the kettle bottom, and then pick up the piece of sheet metal with rags and leaves, being careful not to get burned by the fire burning on the sheet metal, and place the sheet metal, fire and all, on top of the big black kettle.
I stood in awe and disbelief as in a few minutes she removed the sheet metal and took the cookies out of her makeshift oven. The smoke was hanging heavily in the kitchen from the unvented wood fire in the middle of the floor, but the smoke never bothered the hens that were lying on their nests along the inside kitchen wall, and the smoke certainly never interfered with my sampling some of the best-tasting cookies I have ever eaten. That was well worth the whole day in the mountains of Colombia, South America.
From Canalete we traveled north to the coastal town of Los Córdobas, and then north and east following the Caribbean coastline to Puerto Escondido. There are great numbers of refugees taking flight from the neighboring state of Antioquia. That state includes Medellín, the center of the drug-cartel trading business. There is so much violence and abuse of power in that part of the country that families actually leave their farms and flee to towns across state lines for safety and protection of their families and possessions. The drug-cartel thugs simply come to the rural farms and demand chickens or anything else they desire. If a farm family resists they are shot. If they supply the drug cartels, then the government troops come and demand what they would like. If the farmer resists, the troops tell the farmer they know he just gave chickens to the drug lords. That is considered aiding and abetting the enemy, so the troops shoot the farmer and take what they desire anyway.
Not being able to live in a situation like that, the fearful farmers simply abandon their land and buildings and become refugees in their own country—but in a different state.
At all the medical clinics in Colombia, we saw signs that said CAMU, which stands for “Centro de Aténcion Médica de Urgencias” or “Center for Urgent Medical Attention.” We found such a sign at the Puerto Escondido clinic. The clinic serves a population of fifteen thousand and has only one full‑time doctor and one and a half nurses. (I hung around to see what the half nurse looked like, but she never showed up.)
There are ten smaller “clinics” out in the remote rural areas, but most of those never see a real doctor inside their clinic walls.
Puerto Escondido needed an X‑ray machine, all kinds of simple medical supplies, blood-pressure cuffs, thermometers, a birthing table, and lab-analysis equipment. The nurse asked me if I could please find some electric fans to help cool off the one-hundred-plus-degree temperature in the small labor-and-delivery rooms to help mothers in the delivery process.
The kind people at Puerto Escondido offered to prepare us lunch, even though it was about 1:30 in the afternoon. We certainly accepted. While they were busy fixing lunch, we walked down the cement steps to the undeveloped beach area on the shores of the beautiful Caribbean Sea. After lunch we piled back into our Daihatsu four-by-four and headed out again across the magnificently beautiful countryside of Colombia.
On our way from Puerto Escondido to Los Córdobas, the nuns began singing. Soon everyone was trying to sing along as we rode through the countryside. The nuns, Sister Corina and Sister Maria Teresa, were an absolute hoot. At estimated ages of sixty and sixty-five, respectively, they reminded me of a couple of teenage girls on a bus heading to summer camp. They laughed and joked and sang, and I thoroughly enjoyed trying to join in even though I couldn’t understand 95 percent of what was going on.
The clinic at Los Córdobas was the last clinic we visited today. It was getting late in the afternoon, and Father Bernie was making the Daihatsu go just as fast as possible up the hills and across the rough roads in order to keep an appointment he had set for us at 6:00 p.m.
We all were dirty as pigs and windblown from our long day’s journey, but there was no time to go back to the parish house to freshen up. So we drove directly to our appointment with Bishop Molina, the head bishop of the Diocese of Montería.
Next Week: Mission Accomplished in Colombia